Small Bowel MRI (Enterography MRI Protocol and Planning)
Indications for small bowel mri scan
- Low-grade small-bowel obstruction
- Small-bowel masses
- Crohns disease
Contraindications
- Any electrically, magnetically or mechanically activated implant (e.g. cardiac pacemaker, insulin pump biostimulator, neurostimulator, cochlear implant, and hearing aids)
- Intracranial aneurysm clips (unless made of titanium)
- Pregnancy (risk vs benefit ratio to be assessed)
- Ferromagnetic surgical clips or staples
- Metallic foreign body in the eye
- Metal shrapnel or bullet
Patient preparation for Enterography MRI
- A satisfactory written consent form must be taken from the patient before entering the scanner room
- Ask the patient to remove all metal objects including keys, coins, wallet, cards with magnetic strips, jewellery, hearing aid and hairpins
- Ask the patient to undress and change into a hospital gown
- Instruct the patient to hold his or her breath for the breath-hold scans. It's better to coach the patient two to three times before starting the scan.
- Contrast and buscopan injection risk and benefits must be explained to the patient before the scan
- Gadolinium should only be given to the patient if GFR is > 30
- An intravenous line must be placed with extension tubing extending out of the magnetic bore
- Claustrophobic patients may be accompanied into the scanner room e.g. by staff member or relative with proper safety screening
- Offer headphones for communicating with the patient and ear protection
Explain the procedure to the patient and answer questions - Patient should fast for at least six hours
- Note down the weight of the patient
Oral Contrast
The purpose of utilizing an oral contrast agent is to achieve specific signal intensities in the bowel lumen on different types of MRI images. On T2-weighted images, the aim is to produce a high signal intensity in the bowel lumen, while on T1-weighted images, a low signal intensity in the lumen is desired. The low signal intensity on T1-weighted images is particularly crucial for identifying mural enhancement on post-contrast T1-weighted images.
Water alone is insufficient for achieving adequate bowel distention during MR enterography. However, when water is mixed with a solution containing mannitol or sorbitol, better distention can be achieved. Furthermore, the addition of 5ml of Metoclopramide to the mixture significantly enhances the rate of water evacuation from the stomach.
In our department we use the proportion below,
- 2x Oral mannitol 500ml solution
- 5ml of Metoclopramide
We recommend that patients consume a minimum volume of 1 liters of oral contrast, although some patients may find it difficult to comply with this requirement. To ensure proper distal transit, we implement a minimum delay of 30 minutes from the initiation of contrast ingestion to the imaging procedure.
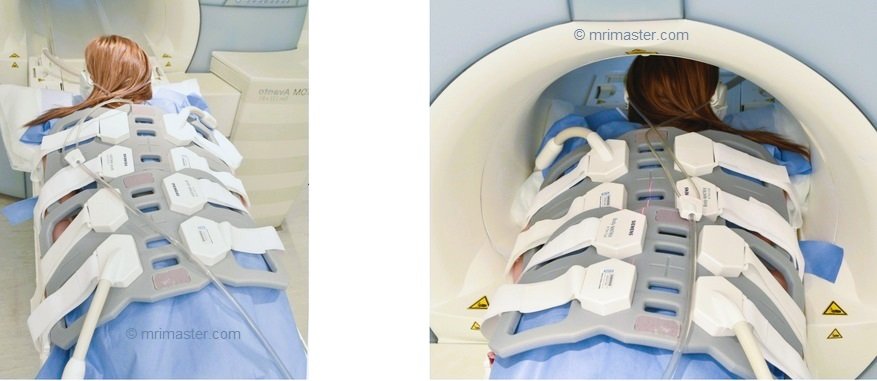
Positioning for for Enterography MRI
- Position the patient in prone position with head pointing towards the magnet (head first prone)
- Position the patient over the spine coil and place the body coils over the upper abdomen and pelvis (nipple down to gluteal crease)
- Securely tighten the body coil using straps to prevent respiratory artefacts
- Give a pillow under the head and cushions under the legs for extra comfort
- Centre the laser beam localiser over iliac crest
Recommended Enterography MRI Protocols and Planning
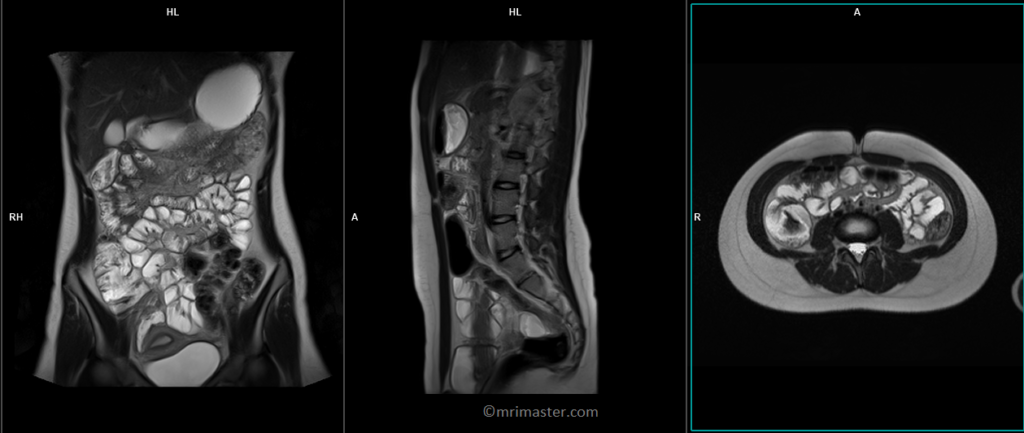
Enterography MRI Localizer
To localize and plan the sequences, it is necessary to obtain an initial three-plane HASTE localizer. These fast single-shot localizers have an acquisition time of under 25 seconds, making them ideal for accurate localization of abdominal structures.
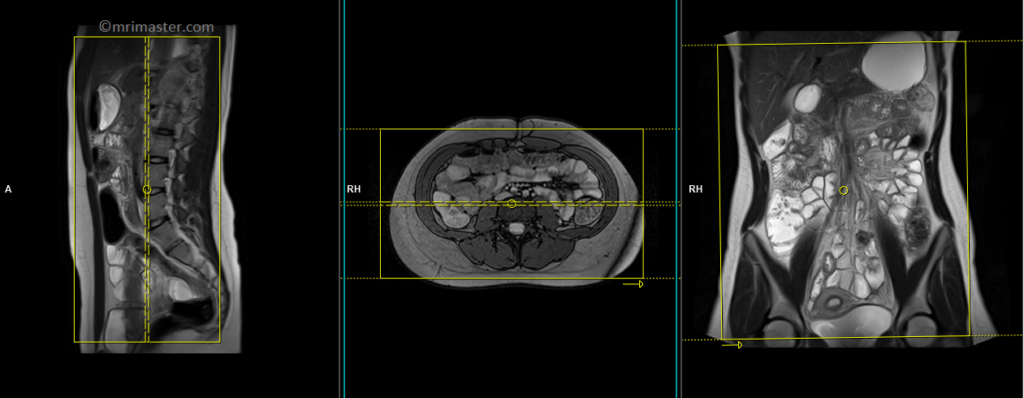
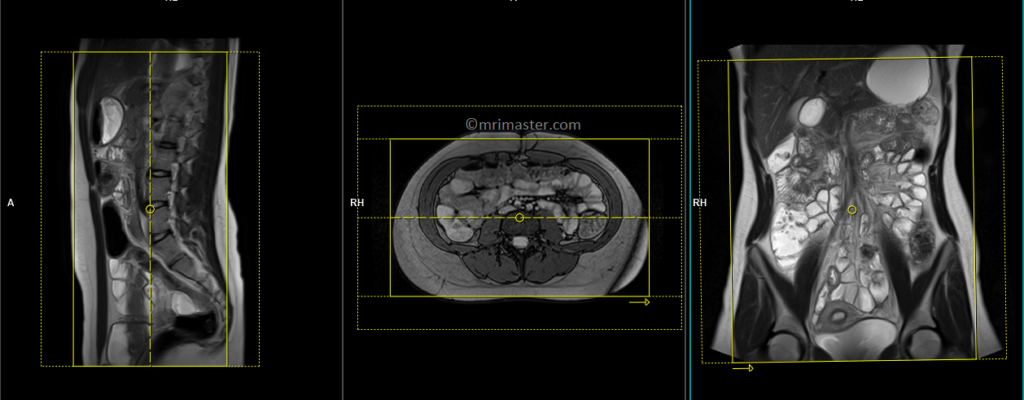
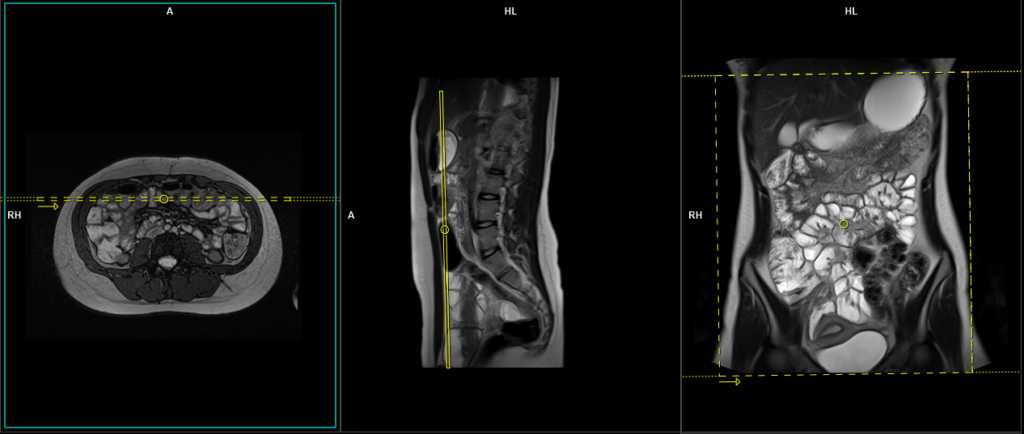
T2 TRUEFISP coronal 4mm
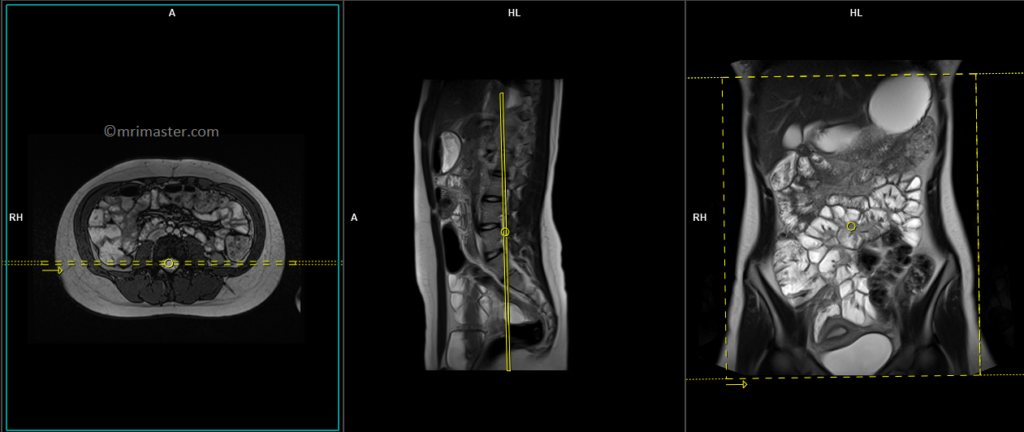
Plan the coronal slices on the axial image. Position the block horizontally across the abdomen as shown, and ensure that the positioning block is also checked in the other two planes. Establish an appropriate angle vertically across the abdomen in the sagittal plane. Make sure the slices adequately cover the entire abdomen, extending from the anterior abdominal wall to the erector spinae muscle. The field of view (FOV) should be large enough to encompass the abdomen and pelvis, ranging from the stomach to the pubic symphysis. To prevent wraparound artifacts, utilize phase oversampling. Instruct the patient to hold their breath during image acquisition. (In our department, we instruct the patients to breathe in and out twice before giving the “breathe in and hold” instruction.)
Protocol Parameters TRUEFISP coronal
TR 4-5 | TE 2-3 | FLIP 60 | NEX 1 | SLICE 4 MM | MATRIX 320×320 | FOV 400-450 | PHASE R>L | OVERSAMPLE 50% | IPAT OFF |
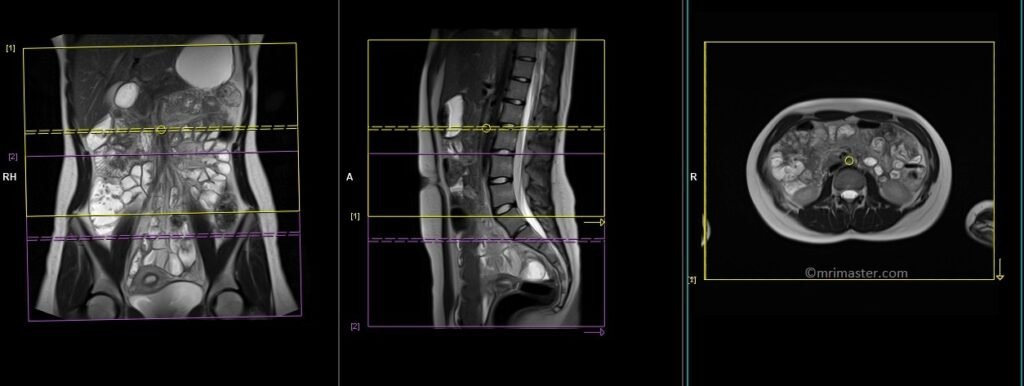
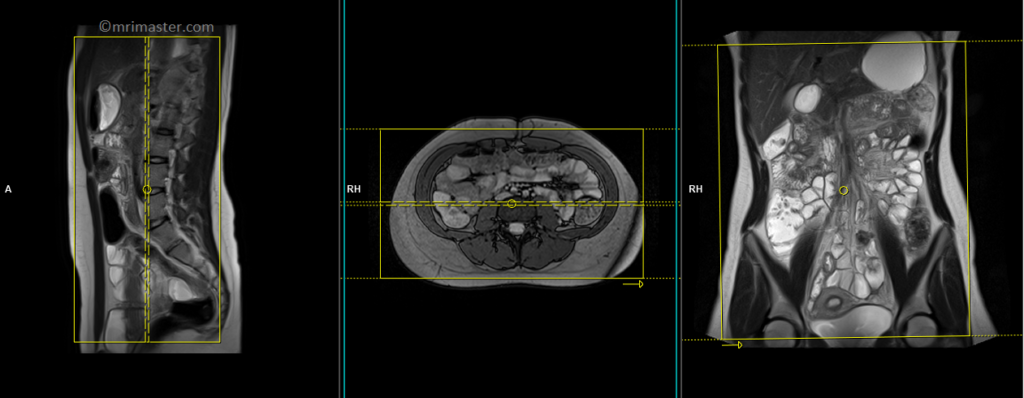
T2 TRUEFISP axial
Plan the axial slices on the coronal image, position the block horizontally across the abdomen as shown, and ensure that the positioning block is also checked in the other two planes. Establish an appropriate angle horizontally across the abdomen in the sagittal plane. The slices must be sufficient to cover the entire abdomen and pelvis from the stomach to the pubic symphysis. Phase oversampling can be used to avoid wrap-around artifacts. Instruct the patient to hold their breath during image acquisition.
The axial scan is performed as two separate blocks with a 20-30% slice overlap between them. The scan is performed this way to avoid any RF inhomogeneity-related artifacts by conducting the scans at the isocenter of the magnet. Use the composing function in the scanner to stitch the two blocks together.
Protocol Parameters TRUEFISP axial
TR 4-5 | TE 2-3 | FLIP 60 | NEX 1 | SLICE 4 MM | MATRIX 320×256 | FOV 350-400 | PHASE A>P | OVERSAMPLE 50% | IPAT ON |
Pause for buscopan injection
Before proceeding to the next step, intravenously inject 0.5 to 1 ml of Buscopan according to the manufacturer’s instructions and departmental policy. Wait for 30 seconds before starting the next scan, as Buscopan takes a few seconds to start its function.
Warning
* Buscopan injection should not be administered to patients with myasthenia gravis, megacolon, narrow-angle glaucoma, tachycardia, prostatic enlargement with urinary retention, mechanical stenoses in the region of the gastrointestinal tract, or paralytic ileus.*
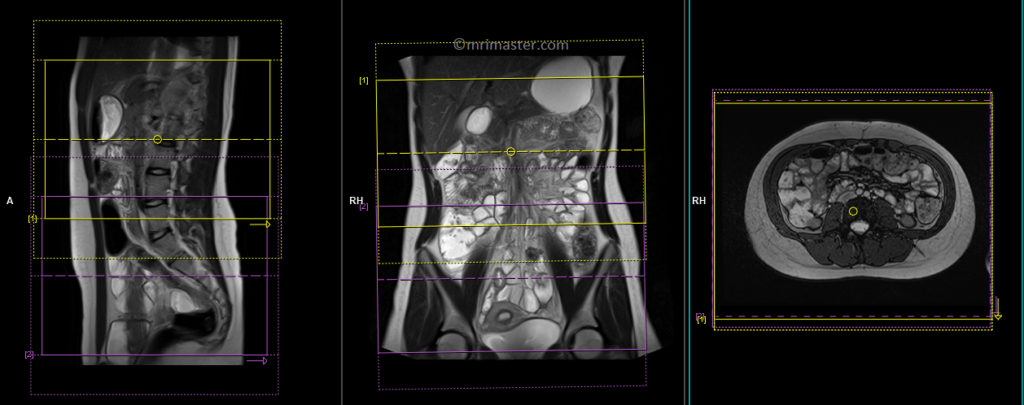
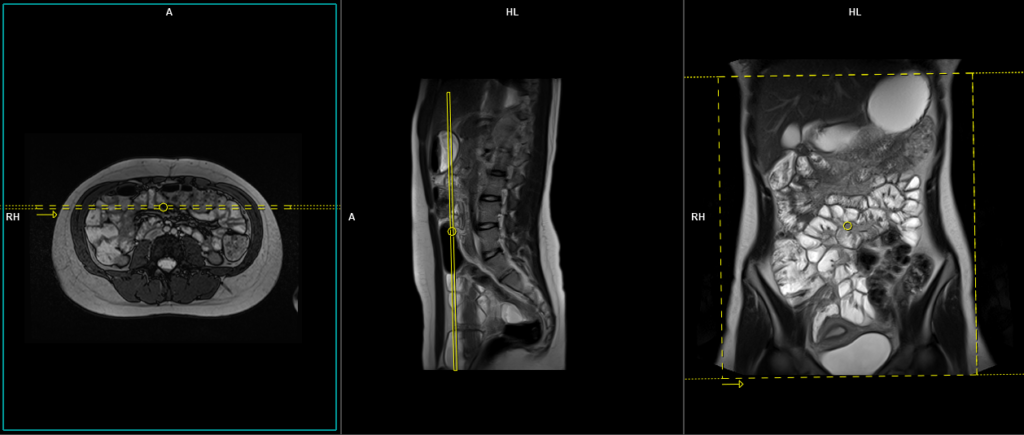
T1 VIBE DIXON \ flash fat sat 3d 0.9-1 mm coronal pre-contrast
Plan the coronal slices on the axial image. Position the block horizontally across the abdomen as shown, and ensure that the positioning block is also checked in the other two planes. Establish an appropriate angle vertically across the abdomen in the sagittal plane. Make sure the slices adequately cover the entire abdomen, extending from the anterior abdominal wall to the erector spinae muscle. The field of view (FOV) should be large enough to encompass the abdomen and pelvis, ranging from the stomach to the pubic symphysis. To prevent wrap-around artifacts, phase oversampling, and in the case of 3D blocks, slice oversampling must be used. Instruct the patient to hold their breath during image acquisition. (In our department, we instruct the patients to breathe in and out twice before giving the “breathe in and hold” instruction.)
Protocol Parameters T1 FLASH Coronal
TR 3-4 | TE 1-2 | FLIP 12 | NEX 1 | SLICE 1 MM | MATRIX 384X320 | FOV 400-450 | PHASE R>L | OVERSAMPLE 50% | IPAT OFF |
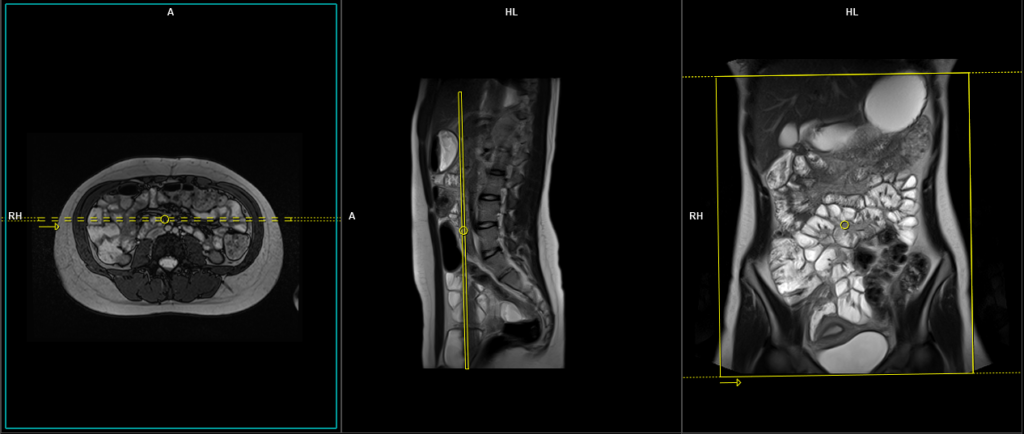
T2 HASTE 4 mm coronal
Plan the coronal slices on the axial image. Position the block horizontally across the abdomen as shown, and ensure that the positioning block is also checked in the other two planes. Establish an appropriate angle vertically across the abdomen in the sagittal plane. Make sure the slices adequately cover the entire abdomen, extending from the anterior abdominal wall to the erector spinae muscle. The field of view (FOV) should be large enough to encompass the abdomen and pelvis, ranging from the stomach to the pubic symphysis. To prevent wraparound artifacts, utilize phase oversampling. Instruct the patient to hold their breath during image acquisition. (In our department, we instruct the patients to breathe in and out twice before giving the “breathe in and hold” instruction.)
Protocol Parameters HASTE Coronal
TR 2000-2500 | TE 90-100 | FLIP 150 | NEX 1 | SLICE 4 MM | MATRIX 320X320 | FOV 400-450 | PHASE R>L | OVERSAMPLE 50% | IPAT ON |
T2 HASTE 4 mm axial
Plan the axial slices on the coronal image, position the block horizontally across the abdomen as shown, and ensure that the positioning block is also checked in the other two planes. Establish an appropriate angle horizontally across the abdomen in the sagittal plane. The slices must be sufficient to cover the entire abdomen and pelvis from the stomach to the pubic symphysis. Phase oversampling can be used to avoid wrap-around artifacts. Instruct the patient to hold their breath during image acquisition.
The axial scan is performed as two separate blocks with a 20-30% slice overlap between them. The scan is performed this way to avoid any RF inhomogeneity-related artifacts by conducting the scans at the isocenter of the magnet. Use the composing function in the scanner to stitch the two blocks together.
Pause for buscopan + gadolinium injection

Protocol Parameters HASTE Axial
TR 2000-2500 | TE 90-100 | FLIP 150 | NEX 1 | SLICE 4 MM | MATRIX 320X320 | FOV 400-450 | PHASE A>P | OVERSAMPLE 0% | IPAT ON |
Before proceeding to the next step, intravenously inject 0.5 to 1 ml of Buscopan (according to the manufacturer’s instructions and departmental policy) and 0.2ml\kg of gadolinium (according to the manufacturer’s instructions and departmental policy). Wait for 30 seconds before starting the next scan (Buscopan takes a few seconds to start its function).
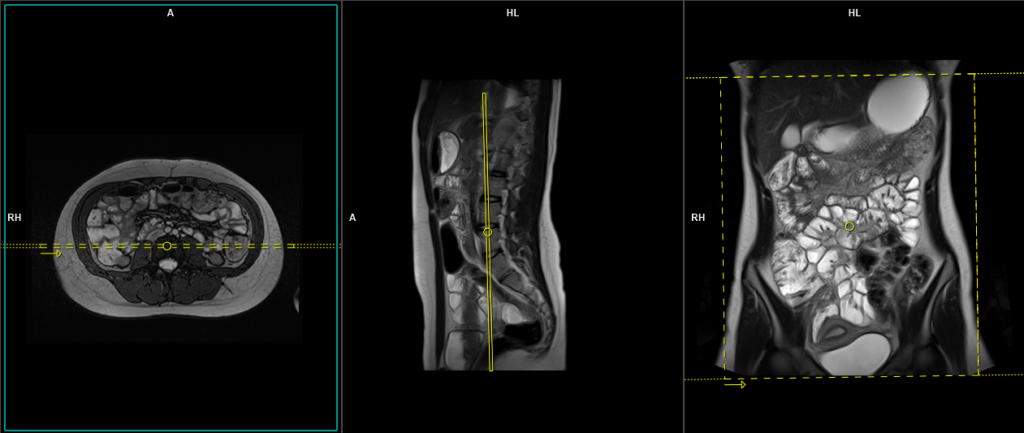
T1 VIBE DIXON \ T1 flash fat sat 3d 0.9-1 mm coronal post contrast
Plan the coronal slices on the axial image. Position the block horizontally across the abdomen as shown, and ensure that the positioning block is also checked in the other two planes. Establish an appropriate angle vertically across the abdomen in the sagittal plane. Make sure the slices adequately cover the entire abdomen, extending from the anterior abdominal wall to the erector spinae muscle. The field of view (FOV) should be large enough to encompass the abdomen and pelvis, ranging from the stomach to the pubic symphysis. To prevent wrap-around artifacts, phase oversampling, and in the case of 3D blocks, slice oversampling must be used. Instruct the patient to hold their breath during image acquisition. (In our department, we instruct the patients to breathe in and out twice before giving the “breathe in and hold” instruction.)
Protocol Parameters T1 FLASH Coronal
TR 3-4 | TE 1-2 | FLIP 12 | NEX 1 | SLICE 1 MM | MATRIX 384X320 | FOV 400-450 | PHASE R>L | OVERSAMPLE 50% | IPAT OFF |
T1 VIBE DIXON \ T1 flash fat sat 3d 1-1.5 mm axial post contrast
Plan the axial slices on the coronal image, position the block horizontally across the abdomen as shown, and ensure that the positioning block is also checked in the other two planes. Establish an appropriate angle horizontally across the abdomen in the sagittal plane. The slices must be sufficient to cover the entire abdomen and pelvis from the stomach to the pubic symphysis. To prevent wrap-around artifacts, phase oversampling, and in the case of 3D blocks, slice oversampling must be used. Instruct the patient to hold their breath during image acquisition. (In our department, we instruct the patients to breathe in and out twice before giving the “breathe in and hold” instruction.)
The axial scan is performed as two separate blocks with a 10-25% slice overlap between them. The scan is performed this way to avoid any RF inhomogeneity-related artifacts by conducting the scans at the isocenter of the magnet. Use the composing function in the scanner to stitch the two blocks together.
Protocol Parameters T1 FLASH Axial
TR 3-4 | TE 1-2 | FLIP 12 | NEX 1 | SLICE 2 MM | MATRIX 320X320 | FOV 350-420 | PHASE A>P | OVERSAMPLE 30% | IPAT ON |
Post Enterography scan complications
Mannitol may lead to certain discomforts in the gastrointestinal tract following the procedure. These discomforts can include diarrhea, excess intestinal gas, and abdominal cramps. These symptoms may persist for a period of 1-2 days after the administration of mannitol.
Buscopan, while generally well-tolerated, can have some temporary side effects. One of the common side effects is blurred vision, which may last for approximately 15 to 30 minutes after the procedure. Additionally, Buscopan has the potential to increase heart rate and may cause dry mouth as well.
Optional Scans
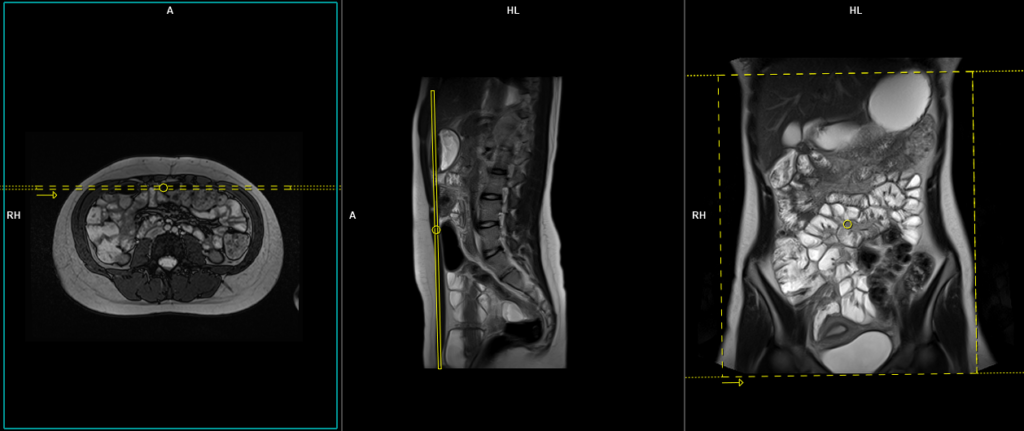
T2 cine coronal 8mm
Multiphasic cine imaging is a crucial element in the assessment of MR enterography, as it offers valuable insights into bowel motility and function. Cine MR enterography is especially beneficial when it comes to examining narrowings and adhesions in the small intestine. Through the evaluation of bowel motility, this imaging method has proven to be advantageous in identifying abnormal lesions associated with conditions such as Crohn’s disease. Its effectiveness has led to its integration into disease activity scoring systems designed for this specific objective.
Cine images are obtained as single slices and can be acquired in any plane. Most commonly, they are acquired in the coronal plane due to the need for fewer slices to cover the entire abdomen. The scanning procedure begins from the anterior abdominal wall and continues by repeating the scan using the stack + function on the scanner until it reaches the sacrum level.
Plan the coronal slice on the axial image. Position the imaging block horizontally across the abdomen as indicated, and ensure that the positioning block is also confirmed in the other two planes. Establish an appropriate vertical angle across the abdomen in the sagittal plane. The field of view (FOV) should be large enough to include the abdomen and pelvis, extending from the stomach to the pubic symphysis. This scan typically takes about 30 seconds to complete and can be performed while the patient breathes freely.
Protocol Parameters True FISP coronal cine
TR 4-5 | TE 2-3 | FLIP 60 | NEX 1 | SLICE 4 MM | MATRIX 320×320 | FOV 400-450 | PHASE R>L | OVERSAMPLE 50% | IPAT OFF |
TR 6000-7000 | TE 90 | IPAT ON | NEX 3 5 8 | SLICE 3 MM | MATRIX 192X192 | FOV 200-250 | PHASE R>L | GAP 10% | B VALUE 0 |
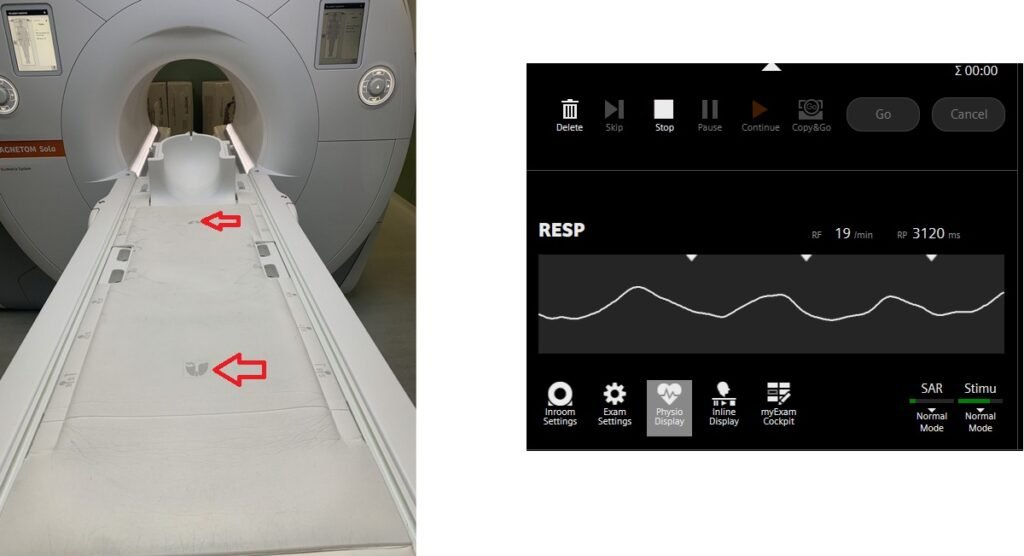
T2 HASTE cornal 5 mm respiratory gated using table respiratory sensor
Respiratory gating in modern scanners can now be accomplished using built-in table respiratory sensors. This feature proves particularly beneficial when patients have irregular breathing patterns or are at risk of falling asleep during the scan. The advantage of table sensors is that they do not necessitate any specific planning. The only requirement is to ensure that the patient’s chest is accurately positioned over the table sensors to enable accurate monitoring of breathing. Additionally, it is important to select the appropriate gating option, such as the table sensor gating, in the protocol settings.
Plan the coronal slices on the axial image. Position the block horizontally across the abdomen as shown, and ensure that the positioning block is also checked in the other two planes. Establish an appropriate angle vertically across the abdomen in the sagittal plane. Make sure the slices adequately cover the entire abdomen, extending from the anterior abdominal wall to the erector spinae muscle. The field of view (FOV) should be large enough to encompass the abdomen and pelvis, ranging from the stomach to the pubic symphysis. Use phase oversampling to prevent wrap-around artifacts. Please advise the patient to maintain a gentle and steady breathing pattern throughout the entire scan.
Parameters
TR 2000-3000 | TE 130 | FLIP 150 | NEX 1 | SLICE 4MM | MATRIX 320X320 | FOV 300-400 | PHASE R>L | OVERSAMPLE 50% | IPAT ON |
Table sensors
Advanced MRI scanners are equipped with built-in table sensors that detect the respiratory waveform and trigger data acquisition during the expiration phase of the respiratory cycle. Proper patient positioning over the sensor is critical for accurate respiratory gating. This method eliminates the need for external respiratory gating equipment, such as sensors and belts.
Unlock MRIMaster Offline & Ad-Free for $10

